Amoxicillin is a semi-synthetic penicillin a close chemical and a pharmacological relative of ampicillin. The drug is stable in acid and is designed for oral use. The antimicrobial spectrum of amoxicillin is essentially identical to that of ampicillin with the important exception that amoxicillin appears to be less effective than ampicillin for shigellosis. Amoxicillin is more rapidly and completely absorbed from the gastrointestinal tract than ampicillin, which is the major difference between the two. Peak concentration in plasma are two to two and one-half times greater for amoxicillin than for ampicillin after oral administration of the same dose. Food does not interfere with absorption, perhaps because of more complete absorption of this congener.
FORMULATION:
Each capsule contains: Amoxicillin (as trihydrate) …………………….. 500 mg
INDICATIONS:
For the treatment of infections caused by susceptible strains of Gram-positive and Gram-negative organisms such as respiratory, G.I. and genito-urinary tracts, skin and soft tissue infections.
PRECAUTION:
Amoxicillin is contraindicated in patients known to be sensitive to penicillin and it should be used with caution in patients with known history of allergy to the drug.
UNDESIRABLE EFFECTS:
Gastrointestinal disturbances and rashes may occur. Small accounts of amoxicillin excreted in the milk may provoke allergic reactions in breastfeed infants.
DOSAGE:
CAPSULE: Adult Dose: One capsule every 6 hours or as prescribed by the physician. SUSPENSION: 1-2 years: 2.5 mL (1/2 teaspoon) 3-6 years: 5 mL (1 teaspoonful) 7-12 years: 5-10 mL (1-2 teaspoonfuls) every 8 hours or as prescribed by the physician.
DIRECTION FOR RECONSTITUTION:
For 250 mg/5 mL Powder for Suspension To make 60 mL reconstituted suspension, mix thoroughly the contents with 45 mL water and shake well until the powder is evenly suspended. The reconstituted suspension is stable for 7 days at temperatures not exceeding 30 degree Celsius and 14 days when refrigerated (2 degree Celsius – 8 degree Celsius).
CAUTION:
Foods, Drugs, Devices and Cosmetics Act prohibits dispensing without prescription.
STORAGE CONDITION:
Store at temperatures not exceeding 30 degree Celsius.
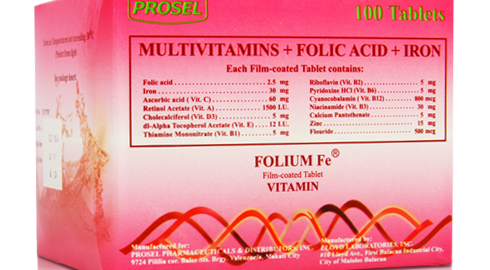
Each tablet contains a high potency formulation of the neurotropic vitamin B1, B6, B12 which is scientifically-based. This pharmacodynamic and neurotropic concentration of Thiamine, Pyridoxine and Cyanocobalamin precisely workds in providing etiologic and symptomatic therapy of painful neurological conditions.
Vitamin E, a fat-soluble vitamin, prevents the oxidation of polyunsaturated fatty acids. It reacts with free radicals, which are the cause of oxidative damage to all membranes, without the formation of another free radical in process.
Vitamin E deficiency is rare but develops when the dietary intake is inadequate. In children with cystic fibrosis or biliary artresia, malabsorption of fat may lead to Vitamin E deficiency; deficiency may occur in children with abnormalities to lipid transport, as in abetalipoproteinaemia. Low vitamin E concentrations are also found in premature, very low birth-weights infants. In previously healthy adults, malabsorption and low intake of vitamin E must continue for number of years before signs of deficiency appear. The major signs of Vitamin E deficiency are the development of myopathic and neurological disorders.
Folic acid is a member of the Vitmain B group, Folic acid is reduced in the body to tetrahydrofolate, which is a coenzyme for various metabolic processes including the synthesis of purine and pyrimidine nucleotides, and hence on the synthesis of DNA: it is also involved in same amino-acid conversion, and in the formation and utilization of formate. Deficiency, which can result in megaloblastic anemia develops when the dietary intake is inadequate (as in malnutrition), when there is malabsorption (asin sprue), increased utilization (as in pregnancy or conditions such as hemolytic anemia), increased loss (as in hemodialysis), or as result of the administration of folate antagonist and other drugs that interfere with normal folate metabolism.
FORMULATION:
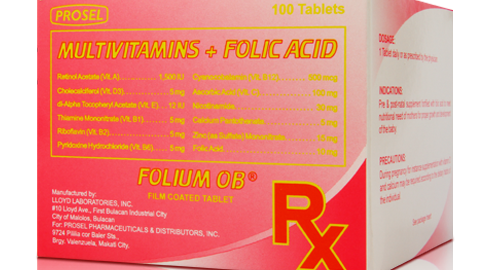
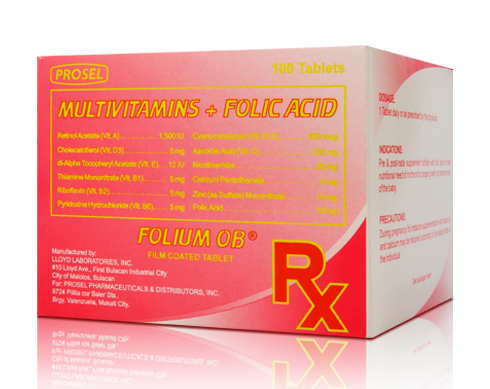
Each film-coated tablet contains: Thiamine Mononitrate (Vit. B1) … 300 mg Pyridoxine HCI (Vit. B6) … 300 mg Cyanocobalamin (Vit. B12) … 1,000 mcg Vitamin E … 100 I.U. Folic acid … 1,000 mcg
INDICATIONS:
Vitamin B-complex is inidicated for the treatment of neuritis, neuralgia, polyneuritis, lumbago, cervical and shoulder-arm syndrome, rheumatic pains, Herpes Zoster, alcoholism, cardiac disorders, diabetic neuropathy, encephalopathies, iatrogenic complications arising from INH, reserpine and phenothiazine therapy.
Vitamin B-complex is inidicated for the prevention and treatment of B1, B6, B12 deficiencies. Also, it aids in appetite stimulation and promotes proper metabolism of carbohydrates and proteins. It increases resistance to stress and meets nutritional needs for Vitamin B1, B6 and B12 of pregnant and lactating mothers, elderly persons and those on special diet.
Vitamin E is used in the treatment and prevention of Vitamin E deficiency.
Folic Acid is used in the treatment and prevention of folate deficiency state. It is also used in women of child-bearing potential and pregnant women to protect against neural tube defects in their offsping.
RECOMMENDED DOSE: For the therapeutic use, 2-4 tablets may be given daily until acute symtoms subside. For chronic cases, longer therapy may be required and dosage may be adjusted upon physician’s recommendation. For prophylactic administration, 1-2 tablets daily is recommended or as prescribed by the physician.
ADVERSE EFFECTS:
The vitamins contained in Vitamin B Complex are completely non-toxic even in high doses and usually, no side effects occur. Sensitivity to Vitamin B1 however may sometimes be encountered if administration is at prolonged intervals, irregular, or if initial dose are low and suddenly increased. Liver dysfunctions could also predispose patients to hypersensitivity reactions. Nevertheless, it must be stressed that hypersensitivity to Vitamin B1 is very rare when orally given unlike if administered by intravenous injection where hypersensitivity is more often encountered.
Vitamin E is usually well tolerated. Large doses may cause diarrhea, abdominal pain and other gastrointestinal disturbances and have also been reported to cause fatigue and weakness.
Folic acid generally well tolerated. Gastrointestinal disturbances and hypersensitivity reactions have been reported rarely.
WARNING:
This product contains FD & C yellow #5 (tartrazine) which may cause allergic type reactions (including brochial asthma) in certain susceptible persons.
CAUTIONS:
Foods, Drugs, Devices and Cosmetics Act prohibits dispensing without prescription.
Vitamin Pre-natal is indicated to provide essential vitamins and supplementation throughout pregnancy and during the postnatal period for both the lactating and non-lactating mother.
CLINICAL PHARMACOLOGY:
Vitamins and minerals are essential for normal metabolic functions including hematopoiesis. The B-complex vitamins are necessary for the conversion of carbohydrate, protein and fat into tissue and energy.
Ascorbic acid is necessary for proper functioning of the retina. It appears to be essential to the integrity of epithelial cells.
Vitamin E is an antioxidant which preserves essential cellular constituents.
Water soluble vitamins (B-complex and C) are not significantly stored by the body and must be replaced continually to maintain essential tissue levels, excess quantities are excreted in the urine. These vitamins are rapidly depleted in condition interferingwith their intake or absorption. Therefore, vitamin preparation should supply therapeutic levels of Vitamin C & B-complex vitamins.
Fat soluble vitamins can accumulate in the body and do not need replacement as frequently. Therefore, vitamin should supply more conservative levels of Vitamins A snd E.
Zinc facilitates wound healing, helps maintains normal growth rates, normal skin hydration and senses of taste and smell.
Calcium pantothenate is produced in the intestines by bacteria and is often nicknamed the anti-stress vitamin, it is known to place a role in preventing depression.
INDICATIONS:
Pre & post-natal supplement fortified with folic acid to meet the nutritional needs of mothers for proper growth & development of the baby.
ADVERSE REACTIONS:
Adverse reactions have been reported with specific vitamins and folic acid generally at levels substantially higher than those in vitamins. However, allergic and idiosyncratic reactions are possible at lower levels.
DOSAGE:
1 Tablet daily or as prescribed by the physician.
STORAGE:
Store at temperature not exceeding 30 degree Celsius.
Prenatal Vitamin is indicated to provide essential vitamin and supplementation throughout pregnancy and during the postnatal period for both the lactating and non-lactating mother.
CLINICAL PHARMACOLOGY:
Vitamins and minerals are essential for normal metabolic function including hematopoiesis. The B-complex vitamins are necessary for the conversion of carbohydrate, protein and fat into tissue and energy. Ascorbic Acid is necessary for proper functioning of the retina; it apears to be essential to the integrity of epithelial cells. Vitamin E is an antioxidant which preserves essential cellular constituents.
Water soluble vitamins (B-complex and C) are not significantly stored by the body and must be replaced continually to maintain essental tissue levels; excess quantities are excreted in urine. These vitamins are rapidly deplted in conditions interfering with their intake or absorption. Vitamins, supplies therapeutic levels of vitamin C & B-complex vitamins.
Fat soluble vitamins can accumulate in the body and do not need replacement as frequently. Therefore, Vitamins supply more conservative levels of Vitamins A and E.
Zinc facilitates wound healing, helps maintains normal growth rates, normal skin hydration and senses of taste and smell.
Calcium pantothenate is produced in the intestines by bacteria and is often nick-named the anti-stress vitamin, as it is known to place a role on preventing depression.
INDICATIONS:
Pre & post-natal supplement fortified with folic acid to meet nutritional need of mothers for proper growth & development baby.
ADVERSE REACTIONS:
Adverse reactions have been reported with specific vitamins and folic acid but generally at levels substantially higher than those in Vitamins. However, allergic and idiosyncratic reactions are possible at lower levels.
DOSAGE:
To be taken once a day for supplement or as prescribed by the physician.
CAUTION:
Food, Drugs, Devices and Cosmetics Act prohibits dispensing without prescription.
STORAGE CONDITION:
Store at temperature not exceeding 30 degree Celsius.
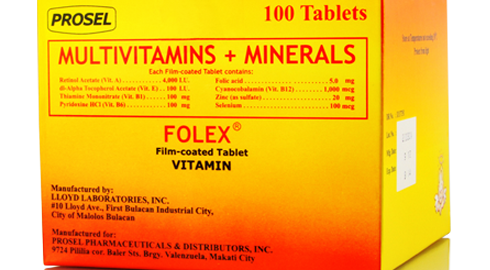
Multivitamins and minerals are indicated to provide essential vitamin supplementation. And to prevent the development of an expected deficiency. Also as a treatment to reduce the risk for diseases like cardiovascular disease.
CLINICAL PHARMACOLOGY:
Vitamins and minerals are essential for normal metabolic functions including hematopolesis. The B-Complex vitamins are necessary for the conversion of carbohydrate, protein and fat into tissue and energy. Vitamin E is an antioxidant which preserves essential cellular constituents.
Folic acid is important in regeneration of blood forming elements.
Water soluble vitamins (B-complex) are not significantly store in the body and must be replaced continually to maintain essential tissue levels; excess quantities are excreted in urine. These vitamins are rapidly depleted in conditions interfering with their intake or absorption. Therefore, vitamin preparation should supply therapeutic levels of B-complex vitamins.
Fat soluble vitamins can accumulate in the body and do not need replacement as frequently. Therefore, vitamin preparations should supply conservative levels of vitamins A and E.
Zinc facilitates wound healing, helps maintains normal growth rates, normal skin hydration and senses of taste and smell.
Selenium activates an antioxidant enzyme called gluthathione peroxidase which help protect the body from cancer. It is also essential for healthy immune functioning.
INDICATIONS:
As vitamin supplement for patients with vitamins and minerals deficiencies. And for patients with cardiovascular diseases with risk of folic acid deficiency.
PRECAUTIONS:
As with any other medication or dietary supplement, vitamin B1 supplements should always be kept well out of reach of children.
ADVERSE REACTIONS:
Adverse reactions have been reported with specific vitamins and folic acid but generally at levels substantially higher than those in vitamins. However, allergic and idiosyncratic reactions are possible at lower levels.
DOSAGE:
1 Tablet daily or as prescribed by the physician.
STORAGE:
Store at temperatures no exceeding 30 degree Celsius.
Prednisolone is a glucocortocoid given, as the free alcohol or in esterified form, orally or parenterally, in the treatment of various disorders in which corticosteroids are indicated, except adrenal deficiency states. Adverse effects are those of corticosteroids in general. It has relatively slight mineralocorticoid effects.
FORMULATION:
Each 5mL (1 teaspoonful) contains: Prednisolone (as sodium phosphate)
PHARMACOKINETICS:
Prednisolone and prednisone are both readily absorbed from the gastrointestinal tract, but whereas prednisolone already exists in metabolically active form, prednisone must be converted in the liver to its active metabolite, prednisolone. In general, this conversion is so that prednisone has a preconversion biological half-life of only about 60 minutes. Hence, although prednisone has been estimated to have only about 80% the bioavailability of prednisolone, this difference is of little consequence when seen in the light of inter-subject variation in the pharmacokinetics of prednisolone itself: bioavailability also depends on the dissolution rates of the tablet formulations. Nevertheless, prednisolone is the more reliably absorbed of the two corticosteroids, particularly in some liver diseases where the conversion of prednisone may be diminshed. Peak plasma concentrations of prednisolone are obtained 1 to 2 hours after administration by mouth, and its plasma half-life is 2 to 4 hours. Its initial absorption, but not its overall bioavailability, is affected by food. Prednisolone is extensively bound to plasma proteins, although less so than hydrocortisone (cortisol). Predisolone is excreted in the urine as free and conjugated metabolities, together with an appreciable proportion of unchaged prednisolone. Prednisolone crosses the placenta and small amounts are excreted in the breast milk.
Prednisolone is excreted in the urine as free and conjugated metabolitites, together with an appreciable proportion of unchanged prednisolone. Prednisolone crosses the placenta and small amounts are excreted in breast milk.
Prednisolone has a biological half-life lasting several hours, intermediate between those of hydrocortisone (cortisol) and the longer acting glucocorticoids such as dexamethasone. It is this intermediate duration of action which makes it suitable for the alternate-day administration regimens which has been found to reduce the risk of adrenocortical insufficiency, yet provide adequate corticosteroid coverage in some disorders.
ADVERSE EFFECTS:
Large doses of corticosteroids, or of corticotropin may produce Cushingold symtoms typical of hyperactivity of the adrenal cortex, with moon face sometimes with hirsutism, bufallo hump, flushing, increased bruising, ecchymoses, striae, and acne, sometimes leading to a fully developed Cushing’s syndrome. If administration is discontinued these symtoms are usually reversed, but sudden cessation is dangerous.
Other adverse effects include amenorrhea, hyperhydrosis, skin thinning, ocular changes including development of cataract, mental and neurological disturbances, intracranial hypertension, acute pancreatitis, and aseptic necrosis of bone. An increase in coagulability of the blood may lead to thromboembolic complications. Peptic ulceration has been of the blood may lead to thromboembolic complications. Peptic ulceration has been reported. Muscle weakness and wasting occur occasionally, particularly when corticosteroids are taken in large doses. The former arises from the mineralocorticoid properties of corticosteroids, the latter from their glucocorticoid properties and is most evident with triamcinolone.
Prednisolone is a glucocortocoid given, as the free alcohol or in esterified form, orally or parenterally, in the treatment of various disorders in which corticosteroids are indicated, except adrenal deficiency states. Adverse effects are those of corticosteroids in general. It has relatively slight mineralocorticoid effects.
Prednisolone and prednisone are both readily absorbed from the gastrointestinal tract, but whereas prednisolone already exists in metabolically active form, prednisone must be converted in the liver to its active metabolite, prednisolone. In general, this conversion is so that prednisone has a preconversion biological half-life of only about 60 minutes. Hence, although prednisone has been estimated to have only about 80% the bioavailability of prednisolone, this difference is of little consequence when seen in the light of inter-subject variation in the pharmacokinetics of prednisolone itself: bioavailability also depends on the dissolution rates of the tablet formulations. Nevertheless, prednisolone is the more reliably absorbed of the two corticosteroids, particularly in some liver diseases where the conversion of prednisone may be diminshed. Peak plasma concentrations of prednisolone are obtained 1 to 2 hours after administration by mouth, and its plasma half-life is 2 to 4 hours. Its initial absorption, but not its overall bioavailability, is affected by food. Prednisolone is extensively bound to plasma proteins, although less so than hydrocortisone (cortisol). Predisolone is excreted in the urine as free and conjugated metabolities, together with an appreciable proportion of unchaged prednisolone. Prednisolone crosses the placenta and small amounts are excreted in the breast milk.
Prednisolone is excreted in the urine as free and conjugated metabolitites, together with an appreciable proportion of unchanged prednisolone. Prednisolone crosses the placenta and small amounts are excreted in breast milk.
Prednisolone has a biological half-life lasting several hours, intermediate between those of hydrocortisone (cortisol) and the longer acting glucocorticoids such as dexamethasone. It is this intermediate duration of action which makes it suitable for the alternate-day administration regimens which has been found to reduce the risk of adrenocortical insufficiency, yet provide adequate corticosteroid coverage in some disorders.
ADVERSE EFFECTS:
Large doses of corticosteroids, or of corticotropin may produce Cushingold symtoms typical of hyperactivity of the adrenal cortex, with moon face sometimes with hirsutism, bufallo hump, flushing, increased bruising, ecchymoses, striae, and acne, sometimes leading to a fully developed Cushing’s syndrome. If administration is discontinued these symtoms are usually reversed, but sudden cessation is dangerous.
Other adverse effects include amenorrhea, hyperhydrosis, skin thinning, ocular changes including development of cataract, mental and neurological disturbances, intracranial hypertension, acute pancreatitis, and aseptic necrosis of bone. An increase in coagulability of the blood may lead to thromboembolic complications. Peptic ulceration has been of the blood may lead to thromboembolic complications. Peptic ulceration has been reported. Muscle weakness and wasting occur occasionally, particularly when corticosteroids are taken in large doses. The former arises from the mineralocorticoid properties of corticosteroids, the latter from their glucocorticoid properties and is most evident with triamcinolone.
Prednisolone is used in physiological doses for replacement therapy in adrenal insufficiency. Pharmacological doses are used when palliative anti-inflammatory or immunosuppressant effects are required.
DESCRIPTION:
Prednisolone is a glucocorticoid given, as the free alcohol or in esterified form, orally or parenterally, in the treatment of various disorders in which corticosteroids are indicated, except adrenal deficiency states, Adverse effects are those of corticosteroids in general. It has relatively slight mineralocorticoid effects.
FORMULATION:
Each film coated tablet contains: Prednisone ……………………………. 50 mg
PHARMACOKINETICS:
Prednisolone and prednisone are both readily absorbed from the gastrointestinal tract, but whereas prednisolone alrealy exists in metabolically active form, prednisone must be converted in the liver to its active metabolite, prednisolone. In general, this conversion is so that prednisone has been estimated to have only about 60 minutes. Hence, although prednisone has been estimated to have only about 80% the bioavailability of prednisolone, this difference is of little consequence when seen in the light of inter subject variation in the pharmacokinetics of prednisoline itself: bioavailabilityalso depends on the dissolution rates of the tablet formulations. Nevertheless, prednisolone is the more reliably absorbed of the two corticosteroids, particularly in some liver diseases where the conversion of prednisone may be diminished. Peak plasma concentrations of prednisolone are obtained 1 to 2 hours after administration by mouth, and its plasma half-life is 2 to 4 hours. Its initial absorption, but not its overall bioavailability, is affected by food.
Prednisolone is extensively bound to plasma proteins, although less so than hydrocortisone (cortisol).
Prednisolone is excreted in the urine as free and conjugated metabolites, together with an appreciable proportion of unchanged prednisolone. Prednisolone crosses the placenta and small amounts are excreted in breast milk.
Prednisolone has a biological half-life lasting several hours, intermediate between those of hydrocortisone (cortisol) and the longer acting glucocorticoids such as dexamethasone. It is this intermediate duration of action which makes it suitable for the alternate-day administration regiments which has been found to reduce the risk of adrenocortical insufficiency, yet provide adequate corticosteroid coverage in some disorders.
ADVERSE EFFECTS:
Large doses of corticosteroids, or of corticotropin may produce Cushingoid symptoms typical of hyperactivity of the adrenal cortex, with moon face sometimes with hirsutism, buffalo hump, flushing, increased bruising, ecchymoses, striae, and acne, sometimes leading to a fully developed Cushing’s syndrome. If administration is discontinued these symptoms are usually reversed, but sudden cessation is dangerous.
Other adverse effects include amenorrhea, hyperhydrosis, skin thinning, ocular changes including development of cataract, mental and neurological disturbances, intracranial hypertension, acute pancreatitis, and aseptic necrosis of bone. An increase in coagulability of the blood may lead to thromboembolic complications. Peptic ulceration has been reported. Muscle weakness and wasting occur occasionally, particularly when corticosteroids are taken in large doses. The former arises from the mineralocorticoid properties of corticosteroids, the latter from their glucocorticoid properties and is most evident with triamcinolone.
PRECAUTION:
The dose of corticosteroid required to diminish corticotropin secretion with consequent atrophy of the adrenal cortex and the time required for its occurence very from patient to patient. Acute adrenal insufficiency may occur during prolonged treatment or on cessation of treatment and may be precipitated by stressful situations. Growth retardation in children has been reported. High doses of corticosteroids administered during pregnancy may cause fetal or neonatal adrenal suppression.
DOSAGE:
The usual dose for prednisolone is 5 to 60 mg daily in divided doses, as a single daily dose after breakfast, as double dose on alternate days, or as prescribed by the physician.
CAUTION:
Foods, Drugs, Devices and Cosmetics Act prohibits dispensing without prescription.
AVAILABILITY:
Prednisolone 50 mg film-coated tablet Blister Pack x 10’s – Box of 30’s
STORAGE CONDITION:
Store at terperatures not exceeding 30 degree Celsius.
Large doses of corticosteroids, or of corticotropin may produce Cushingoid symptoms typical of hyperactivity of the adrenal cortex, with moon face sometimes with hirsutism, buffalo hump, flushing, increased bruising, ecchymoses, striae, and acne, sometimes leading to a fully developed Cushing’s syndrome. If administration is discontinued these symptoms are usually reversed, but sudden cessation is dangerous.
Other adverse effects include amenorrhea, hyperhydrosis, skin thinning, ocular changes including development of cataract, mental and neurological disturbances, intracranial hypertension, acute pancreatitis, and aseptic necrosis of bone. An increase in coagulability of the blood may lead to thromboembolic complications. Peptic ulceration has been reported. Muscle weakness and wasting occur occasionally, particularly when corticosteroids are taken in large doses. The former arises from the mineralocorticoid properties of corticosteroids, the latter from their glucocorticoid properties and is most evident with triamcinolone.
INDICATIONS:
Prednisolone is used in physiological doses for replacement therapy in adrenal insufficiency. Pharmacological doses are used when palliative anti-inflammatory or immunosuppressant effects are required.
DESCRIPTION:
Prednisolone is a glucocorticoid given, as the free alcohol or in esterified form, orally or parenterally, in the treatment of various disorders in which corticosteroids are indicated, except adrenal deficiency states, Adverse effects are those of corticosteroids in general. It has relatively slight mineralocorticoid effects.
FORMULATION:
Each film coated tablet contains: Prednisone ……………………………. 30 mg
PHARMACOKINETICS:
Prednisolone and prednisone are both readily absorbed from the gastrointestinal tract, but whereas prednisolone alrealy exists in metabolically active form, prednisone must be converted in the liver to its active metabolite, prednisolone. In general, this conversion is so that prednisone has been estimated to have only about 60 minutes. Hence, although prednisone has been estimated to have only about 80% the bioavailability of prednisolone, this difference is of little consequence when seen in the light of inter subject variation in the pharmacokinetics of prednisoline itself: bioavailabilityalso depends on the dissolution rates of the tablet formulations. Nevertheless, prednisolone is the more reliably absorbed of the two corticosteroids, particularly in some liver diseases where the conversion of prednisone may be diminished. Peak plasma concentrations of prednisolone are obtained 1 to 2 hours after administration by mouth, and its plasma half-life is 2 to 4 hours. Its initial absorption, but not its overall bioavailability, is affected by food.
Prednisolone is extensively bound to plasma proteins, although less so than hydrocortisone (cortisol).
Prednisolone is excreted in the urine as free and conjugated metabolites, together with an appreciable proportion of unchanged prednisolone. Prednisolone crosses the placenta and small amounts are excreted in breast milk.
Prednisolone has a biological half-life lasting several hours, intermediate between those of hydrocortisone (cortisol) and the longer acting glucocorticoids such as dexamethasone. It is this intermediate duration of action which makes it suitable for the alternate-day administration regiments which has been found to reduce the risk of adrenocortical insufficiency, yet provide adequate corticosteroid coverage in some disorders.
PRECAUTION:
The dose of corticosteroid required to diminish corticotropin secretion with consequent atrophy of the adrenal cortex and the time required for its occurence very from patient to patient. Acute adrenal insufficiency may occur during prolonged treatment or on cessation of treatment and may be precipitated by stressful situations. Growth retardation in children has been reported. High doses of corticosteroids administered during pregnancy may cause fetal or neonatal adrenal suppression.
DOSAGE:
The usual dose for prednisolone is 5 to 60 mg daily in divided doses, as a single daily dose after breakfast, as double dose on alternate days, or as prescribed by the physician.
CAUTION:
Foods, Drugs, Devices and Cosmetics Act prohibits dispensing without prescription.
AVAILABILITY:
Prednisolone 30 mg film-coated tablet Blister Pack x 10’s – Box of 30’s and 100’s
STORAGE CONDITION:
Store at terperatures not exceeding 30 degree Celsius.
Prednisolone is a glucocorticoid given, as the free alcohol or in esterified form, orally or parenterally, in the treatment of various disorders in which corticosteroids are indicated, except adrenal deficiency states, Adverse effects are those of corticosteroids in general. It has relatively slight mineralocorticoid effects.
FORMULATION:
Each film coated tablet contains: Prednisone ……………………………. 20 mg
PHARMACOKINETICS:
Prednisolone and prednisone are both readily absorbed from the gastrointestinal tract, but whereas prednisolone alrealy exists in metabolically active form, prednisone must be converted in the liver to its active metabolite, prednisolone. In general, this conversion is so that prednisone has been estimated to have only about 60 minutes. Hence, although prednisone has been estimated to have only about 80% the bioavailability of prednisolone, this difference is of little consequence when seen in the light of inter subject variation in the pharmacokinetics of prednisoline itself: bioavailabilityalso depends on the dissolution rates of the tablet formulations. Nevertheless, prednisolone is the more reliably absorbed of the two corticosteroids, particularly in some liver diseases where the conversion of prednisone may be diminished. Peak plasma concentrations of prednisolone are obtained 1 to 2 hours after administration by mouth, and its plasma half-life is 2 to 4 hours. Its initial absorption, but not its overall bioavailability, is affected by food.
Prednisolone is extensively bound to plasma proteins, although less so than hydrocortisone (cortisol).
Prednisolone is excreted in the urine as free and conjugated metabolites, together with an appreciable proportion of unchanged prednisolone. Prednisolone crosses the placenta and small amounts are excreted in breast milk.
Prednisolone has a biological half-life lasting several hours, intermediate between those of hydrocortisone (cortisol) and the longer acting glucocorticoids such as dexamethasone. It is this intermediate duration of action which makes it suitable for the alternate-day administration regiments which has been found to reduce the risk of adrenocortical insufficiency, yet provide adequate corticosteroid coverage in some disorders.
ADVERSE EFFECTS:
Large doses of corticosteroids, or of corticotropin may produce Cushingoid symptoms typical of hyperactivity of the adrenal cortex, with moon face sometimes with hirsutism, buffalo hump, flushing, increased bruising, ecchymoses, striae, and acne, sometimes leading to a fully developed Cushing’s syndrome. If administration is discontinued these symptoms are usually reversed, but sudden cessation is dangerous.
Other adverse effects include amenorrhea, hyperhydrosis, skin thinning, ocular changes including development of cataract, mental and neurological disturbances, intracranial hypertension, acute pancreatitis, and aseptic necrosis of bone. An increase in coagulability of the blood may lead to thromboembolic complications. Peptic ulceration has been reported. Muscle weakness and wasting occur occasionally, particularly when corticosteroids are taken in large doses. The former arises from the mineralocorticoid properties of corticosteroids, the latter from their glucocorticoid properties and is most evident with triamcinolone.
PRECAUTION:
The dose of corticosteroid required to diminish corticotropin secretion with consequent atrophy of the adrenal cortex and the time required for its occurence very from patient to patient. Acute adrenal insufficiency may occur during prolonged treatment or on cessation of treatment and may be precipitated by stressful situations. Growth retardation in children has been reported. High doses of corticosteroids administered during pregnancy may cause fetal or neonatal adrenal suppression.
INDICATIONS:
Prednisolone is used in physiological doses for replacement therapy in adrenal insufficiency. Pharmacological doses are used when palliative anti-inflammatory or immunosuppressant effects are required.
DOSAGE:
The usual dose for prednisolone is 5 to 60 mg daily in divided doses, as a single daily dose after breakfast, as double dose on alternate days, or as prescribed by the physician.
CAUTION:
Foods, Drugs, Devices and Cosmetics Act prohibits dispensing without prescription.
AVAILABILITY:
Prednisolone 20 mg film-coated tablet Blister Pack x 20’s – Box of 100’s and 500’s
STORAGE CONDITION:
Store at terperatures not exceeding 30 degree Celsius.